| To Register SMDM Homepage | |

|

|
|
||||
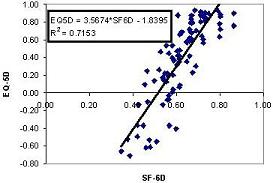
Purpose: Community-derived utility values are recommended for cost-effectiveness analysis and often result in lower health state valuations than patient-derived values. Algorithms have been developed for determining community-derived values, using the SF-6D and EQ-5D, from the SF-12. We assessed within-subject agreement among these community-derived scores and between these scores and patient-derived standard gamble (SG) values for current health. Methods: 92 patients with chronic hepatitis C infection recruited at urban HIV, methadone, and gastroenterology clinics to participate in a survey study completed a computer-assisted standard gamble assessment of current health and the SF-12. Score distributions were compared for one SF-6D algorithm and two EQ-5D algorithms by scatterplot, Pearson correlation coefficient, bivariate linear regression, and intra-class correlation coefficient (ICC). Differences from patient-derived standard gamble values were compared by paired t-test. Results: Score intervals for SF-6D and the 2 EQ-5D algorithms were (0.35-0.86), (0.15-0.98), and (-0.71-0.93). The correlations between the SF-6D and each of the EQ-5D scores were 0.79 and 0.85; agreements by ICC were 0.62 and 0.38. The correlation between the EQ-5D scores was 0.92 and agreement by ICC was 0.73. The mean (SD) differences from patient-derived SG were -0.33 (0.33) for the SF-6D, and -0.14 (0.43) and -0.11 (0.26) for the 2 EQ-5D algorithms. The SF-6D had a significantly greater mean decrement from SG than both EQ-5D algorithms. Conclusions: Because lower boundaries differ between SF-6D and EQ-5D, there is not strong agreement between these scores for poor health states. SF-6D scores indicate greater differences between how community members and patients value health than EQ-5D scores.
See more of Poster Session - Utility Theory; Health Economics; Patient & Physician Preferences; Simulation; Technology Assessment
See more of The 26th Annual Meeting of the Society for Medical Decision Making (October 17-20, 2004)