|
||||


Tuesday, October 23, 2007 - 4:15 PM
G-2
IMPLEMENTATION AND IMPACT OF TWO CANCER SCREENING DECISION AIDS IN PRIMARY CARE PRACTICE
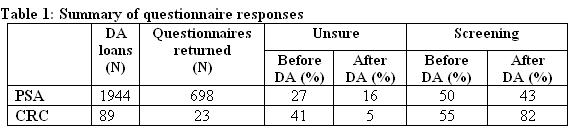
Methods: We systematically distributed PSA and CRC screening video DAs to eligible patients (age 50-75) using three distribution strategies at two academic general internal medicine practices. Patients were asked to watch a PSA or CRC screening DA and complete a pre and post-DA questionnaire. Questionnaires assessed pre/post screening intention, knowledge, values influencing the decision, preference for decision making role and DA acceptability.
Results: 1944 PSA DAs and 89 CRC DAs were distributed over 12 months. After watching DAs:
• A substantial number of patients changed their screening intention (PSA 28%, CRC 35%)
• Fewer patients were unsure about their decision (p < .01)
• Fewer patients preferred to have the PSA test (p < .01)
• More patients indicated they would get screened for colon cancer (p = .03)
• Most patients understood key facts about the decision (PSA 92%, CRC 81%)
• For PSA, more patients chose the screening option predicted by their value scores (71% vs. 57%)
• Patients had clear preference for an active role in decision making (PSA 98%, CRC 95%)
• Patients felt DAs were helpful (PSA 86%, CRC 95%) and would recommend them to others (PSA 95%, CRC 100%)
Provider satisfaction was high with the PSA DA distribution strategy.
Conclusions: A systematic visit based strategy is an effective method to distribute cancer screening DAs. After viewing DAs, patients were well informed, clear about their personal values and prepared to make a decision. Patients found DAs acceptable and would recommend them to others. This process is likely to be appropriate for other preference-sensitive decisions in primary care.